Median Nerve Entrapment, It’s More Than Carpal Tunnel

Nerve entrapment, particularly Carpal Tunnel Syndrome (CTS), is a familiar term for many, but it's just the tip of the iceberg when it comes to conditions affecting the median nerve. In this post, we will chat about nerve compression syndromes of the three main nerves of the arm, shedding light on lesser-known culprits like pronator syndrome and emphasizing the importance of a whole-body approach.
A nerve entrapment syndrome refers to a condition where a peripheral nerve is compressed or irritated, leading to variable symptoms including hand pain, numbness, tingling, or muscle weakness. Most commonly, these entrapments will manifest in the arm or leg and typically won’t have associated spinal pain. Median nerve compression can occur at various points along the nerve's pathway, and the specific symptoms depend on the location and extent of the entrapment.
Three main peripheral nerves supply the arm and forearm: the median, radial, and ulnar nerves. Common examples of entrapment of these nerves include Carpal Tunnel Syndrome, where the median nerve is compressed at the wrist, and Cubital Tunnel Syndrome, involving compression of the ulnar nerve at the elbow. These conditions often result from factors such as repetitive movements, anatomical abnormalities, or prolonged pressure on the nerves.


Beyond the Carpal Tunnel, there are other common sites of nerve injury and associated syndromes such as:
Median Nerve Entrapment Sites:
Pronator Teres Syndrome (PTS): The median nerve can be compressed as it passes through the pronator teres muscle in the forearm. Symptoms may include hand pain, numbness, and tingling in the palm and thumb. In some cases, it may affect the index finger and middle finger, depending on the severity of the nerve compression.
Anterior Interosseous Nerve Syndrome (AINS): AINS involves compression of the anterior interosseous branch of the median nerve. This can lead to weakness in the pinch grip, particularly between the thumb and index finger, although sensory symptoms are minimal. This condition may also indicate an early median nerve injury or underlying nerve damage.
Superficial Palmar Branch Entrapment: Compression of the superficial palmar branch of the median nerve can cause symptoms such as numbness and tingling in the palm or fingers, especially during gripping. In some cases, compression near the transverse carpal ligament may contribute to symptoms in the middle finger and adjacent digits.
Thoracic Outlet Syndrome (TOS): The median nerve can be compressed as it passes through the thoracic outlet (shoulder and neck), leading to symptoms in the arm and hand. Thoracic Outlet Syndrome is a broader nerve entrapment syndrome that can involve compression of multiple structures, including the brachial artery, which may further compromise circulation and function.
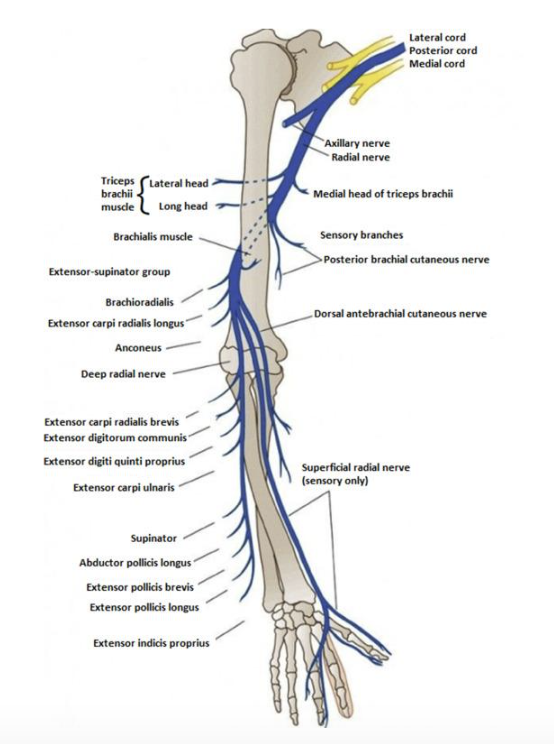
Radial Nerve Entrapment Sites:
Axilla (Axillary Nerve Compression): The radial nerve can be compressed in the axilla (armpit) region, leading to symptoms such as muscle weakness, nerve pain, and functional limitation along the back of the arm. In some cases, nerve conduction studies may be used to confirm the severity of nerve injury or rule out overlapping conditions.
Spiral Groove (Spiral Radial Nerve Compression): As the radial nerve travels down the arm, it courses through the spiral groove of the humerus. Compression at this site can result in nerve entrapment, leading to symptoms such as nerve damage, pain, and weakness in the arm and hand.
Supinator Canal (Arcade of Frohse Compression): The supinator muscle forms a canal known as the supinator canal. Compression of the radial nerve within this canal, also known as the Arcade of Frohse, can lead to radial nerve entrapment syndrome, resulting in symptoms in the forearm that may require physical medicine or physical therapy for recovery.
Wrist (Posterior Interosseous Nerve Compression): The radial nerve divides into the posterior interosseous nerve at the forearm. Compression of this branch at the wrist or proximal forearm can cause muscle weakness and pain in the forearm and hand. In more severe cases, surgical decompression may be required to relieve persistent symptoms and prevent long-term dysfunction.
Ulnar Nerve Entrapment Sites:
Cubital Tunnel (Ulnar Nerve Compression at the Elbow): The cubital tunnel is located on the inner side of the elbow, near the medial epicondyle of the humerus. Compression of the ulnar nerve at this site can lead to Cubital Tunnel Syndrome, causing symptoms such as tingling, muscle weakness, and numbness in the ring and little fingers. In severe or persistent cases, hand surgery may be recommended to relieve pressure and prevent lasting nerve damage.
Guyon's Canal (Ulnar Nerve Compression at the Wrist): Guyon's Canal is situated at the wrist on the palm side. Ulnar nerve compression at this site can result in symptoms like numbness and tingling in the ring and little fingers, often aggravated by gripping or repetitive tasks.
Flexor Carpi Ulnaris (FCU) Arcade: The ulnar nerve may be compressed by the FCU muscle in the forearm, leading to symptoms such as numbness and muscle weakness. This type of nerve entrapment syndrome may coexist with other compression points in the upper limb and may benefit from early physical therapy or, in more advanced cases, surgical decompression.

Why you might be feeling pain or experiencing symptoms in more than one area
Entrapment syndromes can sometimes develop into more radiating-type pain, or there may be concurrent symptoms in the same affected limb, more distal or proximal to the initial site of entrapment. This is known as the Double Crush Phenomenon, which occurs when a nerve, already compressed at one site (like the wrist in carpal tunnel syndrome), becomes more vulnerable if there’s additional compression elsewhere (e.g., neck, shoulder, forearm).
This concept suggests that multiple, even if subclinical or mild, compressions collectively contribute to the overall health of the nerve, potentially leading to median nerve injury, chronic nerve pain, or functional nerve damage. It emphasizes the interconnected nature of nerve pathways and why it is important that treatment considers the whole nerve pathway, rather than looking at one area in isolation.
Diagnosis may involve a nerve conduction study, especially when symptoms are complex or don't resolve with conservative care.

Home Exercises and Stretches
Now that you know a bit more about nerve entrapment, here are some exercises and stretches you can try at home.


In the next videos, we’re demonstrating techniques that mobilise or move each of the nerves discussed in this post. It’s important to note that nerve mobilisation should be gradual, and care should be taken not to “overstretch” these nerves. These movements are often used as part of a broader physical therapy or physical medicine approach to treatment.
Median Nerve Slider
In some instances, it may be too painful to perform the nerve sliding technique on the affected side. If that sounds like you, it might be more beneficial to start by mobilising the nerve on the opposite side.
There are several different levels of nerve mobilisations, so if you are struggling with these nerve sliders, it is important to have this technique tailored to your specific nerve injury by a healthcare professional. It might be that you require additional targeted treatment to the soft tissue structures surrounding your nerve entrapment.
First-line treatment would typically involve a combination of physical therapy, manual therapy, and home-based rehabilitation. In more persistent or severe cases, referral to a physical medicine specialist or consideration of surgical decompression may be warranted, particularly if symptoms suggest progressive nerve damage.
Why Professional Assessment Matters?
Nerve entrapment falls under the umbrella of peripheral neuropathy, which includes conditions that affect the nerves outside the brain and spinal cord. Causes of peripheral neuropathy range from more common nerve compression syndromes to complex systemic or metabolic conditions. For example, rheumatoid arthritis, diabetes, endocrine disorders, and even pregnancy can contribute to nerve damage due to hormonal, inflammatory, or physiological changes.
The duration and nature of symptoms, existing health conditions, and your medical history all play a crucial role in the assessment of entrapment syndromes. Chronic or episodic nerve symptoms, especially when bilateral or affecting multiple sites, may indicate a deeper underlying cause that needs investigation.
Symptoms of median nerve compression or pronator syndrome, for instance, can often mimic or overlap with other conditions, which is why accurate diagnosis is key. This might involve a nerve conduction study or referral to a specialist in physical medicine or hand surgery, depending on the presentation.
Because nerve entrapment syndrome can manifest differently in each person, a thorough clinical evaluation is essential. If you suspect a nerve injury or are experiencing numbness, tingling, hand pain, or muscle weakness, don't delay and seek professional assessment to ensure timely and appropriate treatment.