Why Patellofemoral Pain Becomes Chronic and What Effective Rehab Looks Like

Patellofemoral pain syndrome (PFPS) is a complex, and difficult to diagnose knee injury. It typically arises from overload of the patellofemoral joint, biomechanical abnormalities, or muscular weakness or imbalance. If more than one of these factors are present, PFPS is likely to become chronic. Up to 91% of cases will persist for over 4 years if not treated properly, so correct diagnosis and intervention is crucial.
Because symptoms can mimic other knee conditions, PFPS is frequently misdiagnosed or managed incorrectly, allowing pain to persist for years. Understanding how and why this condition develops is the first step toward effective treatment and long-term recovery.
Summary: This article explains what Patellofemoral Pain Syndrome is, how it develops, and why it can become a long-term issue if not addressed correctly. It outlines the anatomy involved, common causes, how PFPS is diagnosed, and why symptoms often overlap with other knee injuries. You’ll also learn how a structured, progressive rehabilitation approach can reduce pain, restore knee function, and support a safe return to sport or activity.
Surrounding Anatomy
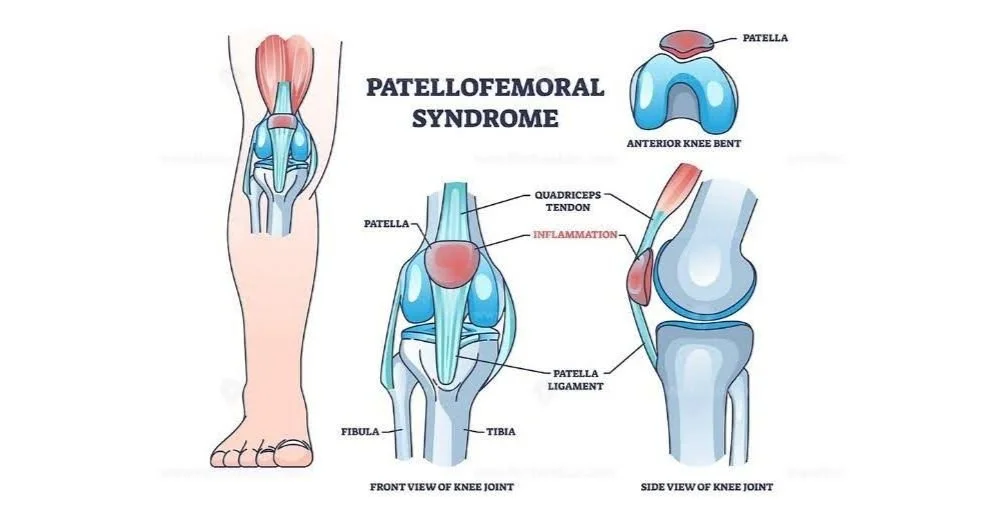
The patella sits within the femoral trochlear groove; with articular cartilage and synovial fluid allowing smooth movement between the surfaces. It is surrounded by various structures; the MCL medially, the LCL laterally and the pre-patellar bursa anteriorly. The patella moves up and down this groove when the knee bends or straightens, although can become inflamed if not able to glide properly.

For the patella to glide properly within the trochlear groove, it requires correct muscle function and alignment from:
The quads muscles (especially the vastus medialis obliquus [VMO])
The lateral soft tissue (such as the ITB)
Hip and core muscles which control lower limb alignment during movement
If this alignment is incorrect, there can be increased stress put onto the patella or surrounding tissues, leading to irritation and pain.
Diagnosing PFPS
PFPS, whilst typically felt exclusively at the patella, can actually be felt all over the knee, and therefore is often misdiagnosed. It has a diagnosis of exclusion; meaning that the condition is diagnosed if:
Pain is felt on or behind the patella when squatting or loading the Patellofemoral Joint (PFJ) in a flexed position
All other knee pathologies have been excluded
Other painful conditions which may be misdiagnosed as PFPS include
Hoffa's pad syndrome
ITB Syndrome
Osteoarthritis in the knee
Baker’s Cyst
How does PFPS present?
Patellofemoral pain syndrome usually arises from a combination of factors, this can include:
Overuse/overload: A sudden increase in load on the knee, such as running distance, squatting, or jumping.
Training errors or surfaces: Other changes in load as seen in running can include changes in training volume, intensity, or surface terrain.
Muscle weakness or imbalance: Poor capacity from the quads or hips to tolerate load can cause the patella to track improperly, and sit outside the trochlear groove
Reduced control: Excessive valgus movement (knees pointing inwards) during walking, running, or squatting can increase patellofemoral load.
Foot and ankle mechanics: Excessive pronation (foot rolling in) or poor footwear can affect positioning of the leg during functional activities, which increase pressure on the knee.
It will tend to feel like a dull ache around or behind the kneecap, which worsens with running, climbing stairs, squatting, or sitting for long periods. Sometimes, it will also present with clicking, grinding, or some feeling of instability.
PFPS is especially common in:
Runners, due to excessive loading of the knee
Cyclists, due to repetitive knee flexion
Team sport players, as a combination of running, jumping, and quick direction changes can cause inflammation in the joint
Young adults/adolescents; especially females, as rapid growth and alignment changes can place the knee under increased load without appropriate muscle support
How do I manage the pain?
Patellofemoral pain doesn’t have to stop you from playing sport and being active — but it requires load management and effective rehab.
Rehabilitation can be split into 3 stages:
1. Acute
- Focus:
Pain management, establish hip/knee control, restore patellar/hip/ankle mobility and restore full range of motion
- Rehab:
Patella mobilisation to increase patella mobility
ART to reduce muscle tightness and adhesions
Patella taping to improve proprioception for patella and medial quads
Dry Needling to increase muscle engagement and reduce tension
Stretching of quads, glutes, hip flexors, ITB and adductors
Strengthening of quads, glutes and core muscles
Exercise examples:
Isometric quads, Straight Leg Raise, Side-lying hip abduction
2. Sub-acute
- Focus:
Progress strength at knee joint and build towards performing closed-chain exercises
- Rehab:
Same interventions as Phase 1 as indicated
Progress strengthening exercises to closed chain, but being careful not to overload
Include some balance/proprioception exercises
Exercise examples:
Strength: Bodyweight box squats, Step ups, Banded crab walks
Proprioception: Single leg stance on Bosu, Star excursion, Flamingo stance
3. Return to sport/activity
- Focus:
Promote correct movement patterns, achieve good strength in all muscle groups, achieve loading through knee flexion with good control and no pain
- Rehab:
Interventions will mostly focus on ART to remove remaining pain/adhesions, and strengthening to increase capacity for load at the knee joint
Progress strengthening exercises to gradually load the PFJ without causing irritation
Correct movement dysfunction with sport-related tasks
Running Assessment and Return to Running programme as required
Exercise examples:
Strength: Goblet squat, Step-downs with eccentric control, Reverse lunge
Proprioception: Single leg squat on Bosu, Banded triplanar toe-taps, Single leg rotations on a balance pad
Will I be able to return to sport pain free?
Yes. PFPS is reversible with the right approach, however, it is often misdiagnosed, and mismanaged. In most cases, symptoms will continue to present for 4+ years. Gradual progression, loading, consistency, and movement quality are crucial components to a successful rehab which will allow you to return to full function.
Patellofemoral Pain Syndrome does not have to be something you simply “push through.” With accurate diagnosis, proper load management, and targeted rehabilitation, most people can return to pain-free movement and sport.
If knee pain has been lingering or limiting your performance, a tailored assessment and rehab plan can make all the difference. Book an appointment with us at Elite Health & Performance to address the root cause and start rebuilding strength, control, and confidence in your knee.
Key Takeaways
Patellofemoral Pain Syndrome is often caused by a combination of overload, muscle weakness, and poor movement control rather than a single injury.
Symptoms can be widespread around the knee, which is why PFPS is frequently misdiagnosed.
Early and accurate diagnosis is critical, as untreated PFPS commonly becomes chronic.
Rehabilitation should be progressive, focusing on strength, movement quality, and gradual loading.
With the right approach, PFPS is reversible and most people can return to sport pain free.
FAQ
How long does Patellofemoral Pain Syndrome take to recover?
Recovery time varies, but many people see improvement within 8 to 12 weeks when following a structured rehab program. Long-standing cases may take longer and require careful load progression.
Should I stop exercising if I have PFPS?
Not usually. Complete rest is rarely recommended. Modifying activity and managing load while continuing appropriate exercise is often more effective than stopping altogether.
Is PFPS the same as runner’s knee?
Yes. Runner’s knee is a common term used to describe Patellofemoral Pain Syndrome, although it can affect non-runners as well.
Can PFPS come back after treatment?
It can if contributing factors such as strength deficits or poor movement patterns are not fully addressed. Ongoing strength work and good load management help reduce recurrence.
Do I need imaging for PFPS?
Imaging is not always required. PFPS is a diagnosis of exclusion, meaning it is identified once other knee pathologies have been ruled out through clinical assessment.